Cardiac Arrest Symptoms and Causes
Cardiac Arrest is the sudden loss of cardiac function, when the heart abruptly stops beating. A person whose heart has stopped will lose consciousness and stop normal breathing, and their pulse and blood pressure will be absent. Unless resuscitative efforts are begun immediately, cardiac arrest leads to death within a few minutes. This is often referred to by doctors as, “sudden death” or “sudden cardiac death.
Ventricular Fibrillation is the most common cause of cardiac arrest. Ventricular fibrillation occurs when the normal, regular, electrical activation of heart muscle contraction is replaced by chaotic electrical activity that causes the heart to stop beating and pumping blood to the brain and other parts of the body. Permanent brain damage and death can occur unless the flow of blood to the brain is restored within five minutes. Heart attack is the most common cause of ventricular fibrillation. Less common causes of cardiac arrest include respiratory arrest (loss of breathing function), choking, trauma, electrocution, and drowning.
Cardiopulmonary Resuscitation (CPR) and Defibrillation (electrical impulses delivered to the chest to restore normal heart rhythm) are the only way to reverse a cardiac arrest. These lifesaving measures must be instituted within a few minutes after cardiac arrest in order to have any chance of success. For every minute that passes without defibrillation, a person’s chances of survival decrease by 7% to 10%. In areas where emergency medical services are able to provide defibrillation within five to seven minutes, the survival rate for cardiac arrest has been reported to be as high as 49%. It is rare for a resuscitation to be successful if more than ten minutes have elapsed following a cardiac arrest.
A heart attack (myocardial infarction) occurs when a portion of the heart muscle dies due to lack of blood flow and oxygen to a specific area of the heart. While having coronary artery disease or having a heart attack can increase a person’s risk for having cardiac arrest, a heart attack is not the same thing as cardiac arrest.. Symptoms of a heart attack typically include chest or other upper body discomfort and shortness of breath. A heart attack can precipitate sudden onset of ventricular fibrillation and cardiac arrest. Heart attack victim that develops ventricular fibrillation will lose consciousness.
Cardiac arrest is obviously a serious medical emergency. The mortality (death rate) from cardiac arrest can be decreased by providing immediate CPR and prompt defibrillation. Many public places are now equipped with automated external defibrillators (AEDs) that allow lay persons to provide emergency defibrillation in case of cardiac arrest.
Being Prepared Can Save a Young Life
Most occurrences of SCA in youth occur in public places. The increased availability of publicly accessible automated external defibrillators (AEDs) in schools and school-sponsored athletic events will dramatically increase the probability that youth will survive SCA. Knowing and properly executing the critically time-urgent links of the Cardiac Chain-of-Survival can help save the life of a youth in SCA.
A sudden blow to the chest when the heart is electrically recharging (between heartbeats) can trigger SCA. The injury is called Commotio Cordis, Latin for “commotion or disturbance of the heart.” Chest protectors do not protect youth from SCA while playing sports and thus create a false sense of security. Chest protectors are designed primarily to protect a child from soft tissue damage and bone injury on impact, not as protection from the potentially fatal heart rhythm that can also occur as a result. Defibrillation (use of AED) is the only effective treatment for a youth struck by Commotio Cordis.
Medical Author: Melissa Conrad Stöppler, MD
Medical Editor: Dennis Lee, MD
REFERENCES: American Heart Associatio. Fauci, Anthony S., et al. Harrison’s Principles of Internal Medicine. 17th ed. United States: McGraw-Hill Professional, 2008. Center for Disease Control (CDC) National Vital Statistics Report for 2005, published April 2008, Volume 56, Number 10
Sudden Cardiac Death Statistics
United States
Each year, 326,200 people in the U.S. experience EMS-assessed out-of-hospital non-traumatic SCA, and nine out of 10 victims die. This is roughly equivalent to the number of people who die from Alzheimers’ disease, assault with firearms, breast cancer, cervical cancer, colorectal cancer, diabetes, HIV, house fires, motor vehicle accidents, prostate cancer and suicides combined. In fact, the incidence of sudden cardiac death is nearly 10 times higher than the incidence of death from breast cancer.
In several population-based studies, the incidence of out-of-hospital cardiac arrest has been noted as declining in the past 2 decades, but the proportion of sudden CAD deaths in the United States has not changed. A high incidence of SCD occurs among certain subgroups of high-risk patients (congestive heart failure with ejection fraction < 30%, convalescent phase after myocardial infarction, patients who survived cardiac arrest). However, these populations are much smaller than patients with minimal or even inapparent coronary artery disease. Consequently, in the overall population, most SCD occurs in lower risk patients. The time dependence of risk for SCD has been noted in several studies, with an increased number of events in the first 6-24 months after surviving a major cardiovascular event.
International
The frequency of SCD in Western industrialized nations is similar to that in the United States. The incidence of SCD in other countries varies as a reflection of the prevalence of coronary artery disease or other high-frequency cardiomyopathies in those populations. The trend toward increasing SCD events in developing nations of the world is thought to reflect a change in dietary and lifestyle habits in these nations. It has been estimated that SCD claims more than 7,000,000 lives per year worldwide. [2]
Mortality/Morbidity
Of more than 300,000 deaths attributed to SCD in the United States each year, a large portion (as many as 40%) are unwitnessed. For most people who experience SCD, their survival depends on the presence of individuals who are competent in performing basic life support, the rapid arrival of personnel and apparatus for defibrillation and advanced life support, and transfer to a hospital. Even under ideal circumstances, only an estimated 20% of patients who have out-of-hospital cardiac arrest survive to hospital discharge. In a study of out-of-hospital cardiac arrest survival in New York City, only 1.4% of patients survived to hospital discharge. Other studies in suburban and rural areas have indicated higher rates of survival (as high as 35%). Placement of automatic external defibrillators throughout communities and training people to use them has the potential to markedly improve outcomes from SCD.
- Upon emergency department (ED) presentation, the most important determinants of survival include (1) an unsupported systolic blood pressure (SBP) greater than 90 mm Hg, (2) a time from loss of consciousness to return of spontaneous circulation (ROSC) of less than 25 minutes, and (3) some degree of neurological responsiveness.
- A major adverse outcome from a SCD event is anoxic encephalopathy, which occurs in 30-80% of cases.
Race
Most studies demonstrate inconclusive data with regard to racial differences as they relate to the incidence of sudden death. Some studies suggest that a greater proportion of coronary deaths were “sudden” in blacks compared to whites. In a report by Gillum et al on SCD from 1980-1985, the percentage of coronary artery disease deaths occurring out of the hospital and in EDs was found to be higher in blacks than in whites (see the image below). [3]
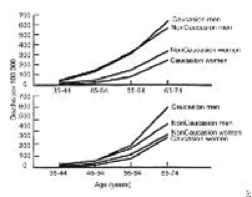
Cardiac death, sudden. Plots of mortality rates (deaths per 1000 persons) for ischemic heart disease occurring out of the hospital or in the emergency department (top) and occurring in the hospital (bottom) by age, sex, and race in 40 states during 1985.
Sex
Men have a higher incidence of SCD than women, with a ratio of 3:1. This ratio generally reflects the higher incidence of obstructive coronary artery disease in men. Recent evidence suggests that a major sex difference may exist in the mechanism of myocardial infarction. Basic and observational data point to the fact that men tend to have coronary plaque rupture, while women tend to have plaque erosion. Whether this biologic difference accounts for the male predominance of SCD is unclear.
Age
The incidence of SCD parallels the incidence of coronary artery disease, with the peak of SCD occurring in people aged 45-75 years. The incidence of SCD increases with age in men, women, whites, and nonwhites as the prevalence of coronary artery disease increases with age. However, the proportion of deaths that are sudden from coronary artery disease decreases with age. In the Framingham study, the proportion of coronary artery disease deaths that were sudden was 62% in men aged 45-54 years, but this percentage fell to 58% in men aged 55-64 years and to 42% in men aged 65-74 years. [4] According to Kuller et al, 31% of deaths are sudden in people aged 20-29 years. [5]
Reference: Medscape Reference 2011 by WebMD LLC.